


















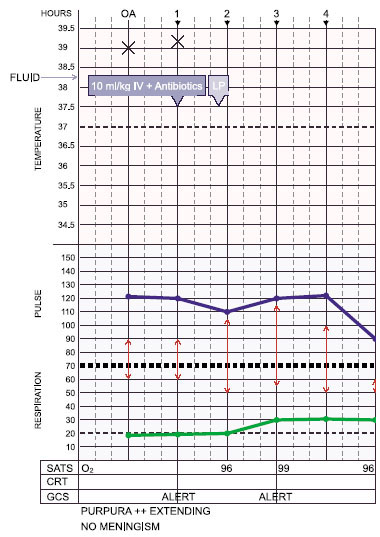
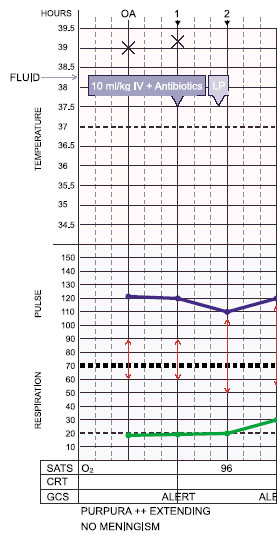
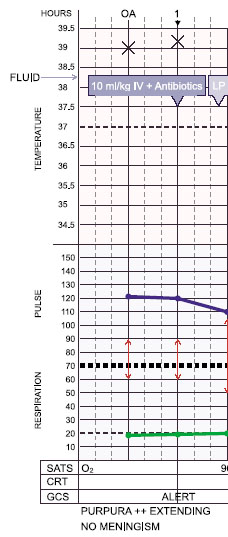







- Rapid fluid resuscitation should be initiated. Boluses of 20ml/kg of colloid (preferably 4.5% albumin44) or crystalloid solutions should be given rapidly (over 5-10 minutes) whilst monitoring the clinical response (HR, RR, BP, CRT, O2 sats, urine output, conscious level). If the clinical response is short-lived or absent, and shock does not improve or progresses, large volumes may be required (over 60ml/kg in the first hour).

Bloated appearance due to capillary leak syndrome. Fluids given during volume resuscitation contribute to this at first.
There is evidence from adults that early goal-directed resuscitation of patients with septic shock is associated with an improvement in outcome45. - Hypoglycaemia (<3.3 mmol/l) is common and should be corrected: 5ml/kg 10% dextrose bolus i.v., then check glucose hourly and correct if necessary.
- If signs of shock persist after 40-60 ml/kg of fluid resuscitation, there is significant risk of pulmonary oedema, so elective tracheal intubation and mechanical ventilation should be initiated even if there are no signs of respiratory failure3. This will optimise oxygenation, reduce the work of breathing, and improve cardiac function.
- Advice to guide further management should be sought early.
- Invasive monitoring and central venous access will be required to guide fluid therapy and optimise support.
- Inotropic support may be required to optimise tissue perfusion and improve myocardial function.
- Metabolic acidosis is common and impairs myocardial contractility. If pH<7.2 due to base deficit, give half correction NaHCO3 iv.
- Volume (ml) to give = (0.3 x weight in kg x base deficit ÷2) of 8.4%NaHCO3 over 20 mins.
- In neonates, volume (ml) to give = (0.3 x weight in kg x base deficit) of 4.2% NaHCO3.
- Metabolic derangements of calcium, magnesium and potassium are common, and need frequent checking and correction .
- In cases of severe bleeding or profound clotting disorder, consider correction of coagulopathy with fresh frozen plasma, platelets and, if fibrinogen is low, cryoprecipitate. Correction of thrombocytopaenia is not generally required, but if uncontrolled haemorrhage from venepuncture sites or mucous membranes occurs despite replacement of clotting factors, platelet transfusion may be required if platelets are below 50,000/mm3.

Dobutamine can be infused centrally or peripherally
Remember – Call for senior help early. Sick septic children need experienced doctors. This is not the time to ‘have a go!’



























