Diagnosis: meningococcal septicaemia. Bloods sent for FBC, biochemistry, U&E, clotting.
(click for larger graph)
Diagnosis: meningococcal septicaemia. Bloods sent for FBC, biochemistry, U&E, clotting.
(click for larger graph)
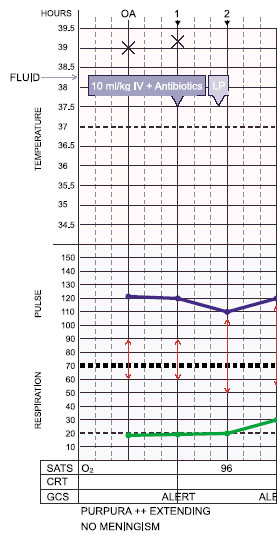
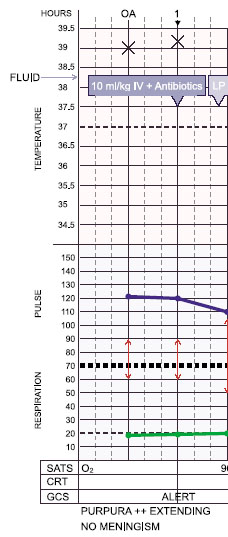
Diagnosis: meningococcal septicaemia. Bloods sent for FBC, glucose, biochemistry, U&E, clotting.
15 year old boy non-specifically unwell for a day. Woke with a widespread purpuric rash and taken straight to hospital. (click for larger graph)
ED assessment: Temp 39.0, HR 120, RR 20, BP 90/60.
Alert no meningism; purpuric rash spreading.
QUESTIONS ON CASE 4
Q 5 of 18: Signs of shock? (Choose one)
YesNoUnknown: not enough clinical parameters have been measured
INCORRECT : Signs of shock: tachycardia, increasing tachypnoea, and hypotension on admission, coexisting with spreading purpuric rash, increasing pyrexia.
Septicaemia will lead to shock and multiorgan failure. Shock is a clinical diagnosis. The signs are a result of circulatory failure. The underlying pathophysiology of septicaemia and the capillary leak syndrome leading to these signs are briefly summarised in the pathophysiology section.
A child in early shock may still be alert and have a normal blood pressure. Child lucid despite advancing septicaemia
The early signs of shock include:
Tachycardia
Cool peripheries (CRT>4 seconds) or toe-core temperature gap of >3 degrees
Pallor, mottling
Decreased urine output (<1ml/kg/hr)
Tachypnoea – secondary to acidosis and hypoxia
(In patients with meningococcal disease, signs of shock will usually co-exist with symptoms of septicaemia.)
As shock progresses further signs develop:
Metabolic acidosis with base deficit worse than -5
Hypoxia: PaO2 <10kPa in air or saturation < 95% in air
Increasing tachypnoea, tachycardia and gallop rhythm