Hb 11.5, WCC 4.3, Platelets 50.
Na 136, K 3.4, urea 6.2, creatinine 138.
Diagnosis: meningococcal septicaemia. Bloods sent for FBC, biochemistry, U&E, clotting.
(click for larger graph)
Diagnosis: meningococcal septicaemia. Bloods sent for FBC, biochemistry, U&E, clotting.
(click for larger graph)
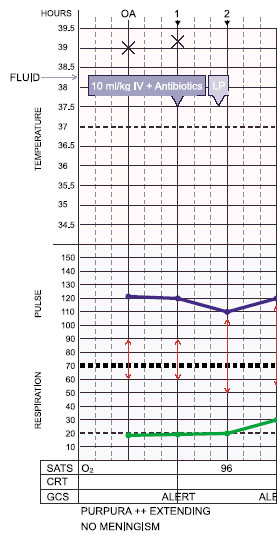
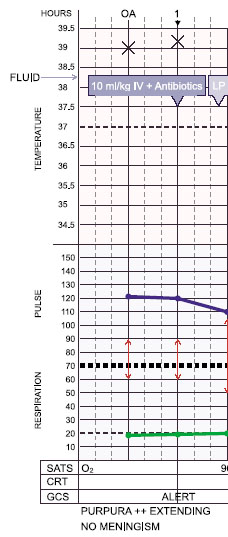
Diagnosis: meningococcal septicaemia. Bloods sent for FBC, glucose, biochemistry, U&E, clotting.
15 year old boy non-specifically unwell for a day. Woke with a widespread purpuric rash and taken straight to hospital. (click for larger graph)
ED assessment: Temp 39.0, HR 120, RR 20, BP 90/60.
Alert no meningism; purpuric rash spreading.
QUESTIONS ON CASE 4
Q 7 of 18: An LP was done during the second hour after admission. Was this appropriate given the clinical signs and the fact that clotting results were not yet available?
Yes No
INCORRECT : An LP was absolutely contraindicated: this was an ill child with a widespread purpuric rash which is strongly suggestive of coagulopathy
(this was later confirmed on blood tests).
Further Information
Lumbar Puncture
Lumbar puncture can be important for treatment if the clinical diagnosis is
in doubt particularly, in children who are febrile without a focus. For children
with obvious meningeal symptoms, microbiological confirmation is valuable for
duration of treatment
decisions about prophylaxis and public health management,
follow up care of children who recover with neurological sequelae, and
disease surveillance.
However, LP must not be performed when there are contraindications and should
never delay treatment. With modern PCR techniques, CSF samples may still be
positive after antibiotics have killed the organisms.
Check with a senior colleague if you are unsure.
Before attempting lumbar puncture assess HR, RR, BP, CRT, pupils, rash, fundal examination for papilloedema.
Make sure there are no signs of raised intracranial pressure or shock.